There is significant room for improvement in the evaluation of hospital-based violence prevention programs. To aid in this pursuit, we have constructed a violence prevention informatics program, with the aid of the software company, QuesGen. An abstract of the work appears below. This program is being considered for wider use and has been demonstrated to the Hospital-Based Violence Intervention Program Conference.
 The National Trauma Data Bank was developed for research and to standardize the process of evaluating the efficacy and quality of trauma centers. Hospital-based violence prevention (VP) programs have been implemented in many trauma centers. However, variables necessary to evaluate and assess programmatic quality are not woven into the trauma registry data. Our objective was to create a "culturally competent" database for both front-end users: the case managers, and for back-end users: researchers and QA personnel. Our goal was to successfully incorporate this into our VP program at two participating sites.
The National Trauma Data Bank was developed for research and to standardize the process of evaluating the efficacy and quality of trauma centers. Hospital-based violence prevention (VP) programs have been implemented in many trauma centers. However, variables necessary to evaluate and assess programmatic quality are not woven into the trauma registry data. Our objective was to create a "culturally competent" database for both front-end users: the case managers, and for back-end users: researchers and QA personnel. Our goal was to successfully incorporate this into our VP program at two participating sites.
Variables to capture quantitative and qualitative data were proposed and modified over a 12-month period. Proposals were initiated by both front end and back end users at both institutions and evaluated for relevance, ease of data entry, and capacity for analysis by all stakeholders. It was created with a Software as a Service solution on a LAMP platform. Each user has a security profile to allow or restrict access and restrict data for HIPPA compliance.
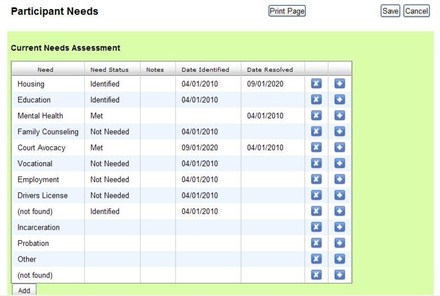
Acceptable quantitative variables that were developed and institutionalized at both level 1 trauma centers included capture rate, needs assessment/risk factors, psychosocial structure, case management time spent, and long-term outcome measures. Qualitative variables implemented included graded quality of client/case manager relationship over time, and notes. Between the two trauma centers, the standardized database has captured 949 trauma patients through its link to the registries, recorded 333 eligible and enrolled 191 clients. Case managers have maintained records on all their clients completely electronically. Back end users can access all data on a spreadsheet and automatic queries can be run in seconds. A sample screen is shown on the right.
Standardized data entry and evaluation of VP programs has lagged behind program development. We have codified a platform for capturing variables relevant to quality assurance and research for VP programs. This system was created in partnership with two level 1 trauma centers to assure exportability. It reflects cultural competency critical for VP programs by creating a user friendly data entry system with input from case managers. It allows for facile download of data for research and quality assurance personnel.
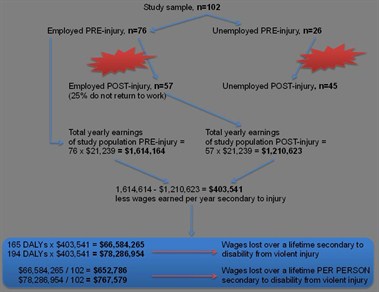 Violent injury devastates urban underserved populations, but the impact over a lifetime is not well characterized. The disability-adjusted life year (DALY) measures the burden of disability and is used widely to describe the long-term impact of a particular disease or injury. The objective of this study was to calculate DALYs and lost wages attributable to violence and its consequences on physical and mental health.
Violent injury devastates urban underserved populations, but the impact over a lifetime is not well characterized. The disability-adjusted life year (DALY) measures the burden of disability and is used widely to describe the long-term impact of a particular disease or injury. The objective of this study was to calculate DALYs and lost wages attributable to violence and its consequences on physical and mental health.